Tongue Tie in Babies: Signs, Symptoms, Treatment and How Osteopathy Can Help
As a Principal Osteopath working with babies every week, tongue tie is something we encounter regularly in clinic. Many parents arrive feeling exhausted, worried and frustrated after struggling with feeding, often having been given conflicting information about whether their baby has a tongue tie and what should be done about it.
One of the biggest misconceptions is that tongue tie is simply a problem with the tongue itself. In reality, feeding difficulties are often much more complex. While a tongue tie may be part of the picture, we frequently find associated tension through the jaw, neck, shoulders and upper body. Factors such as a baby's position in the womb, a difficult birth, assisted delivery, prolonged labour or simply the physical pressures of birth can all contribute to feeding challenges.
When a tongue is unable to move freely, babies often develop compensatory feeding strategies using the jaw, lips and neck muscles. These adaptations can sometimes be just as important as the tongue tie itself when understanding why a baby is struggling to feed. This is one of the reasons we look beyond the mouth and assess the whole baby.
As osteopaths, our role is to look at the whole baby, not just the tongue.
What Is a Tongue Tie?
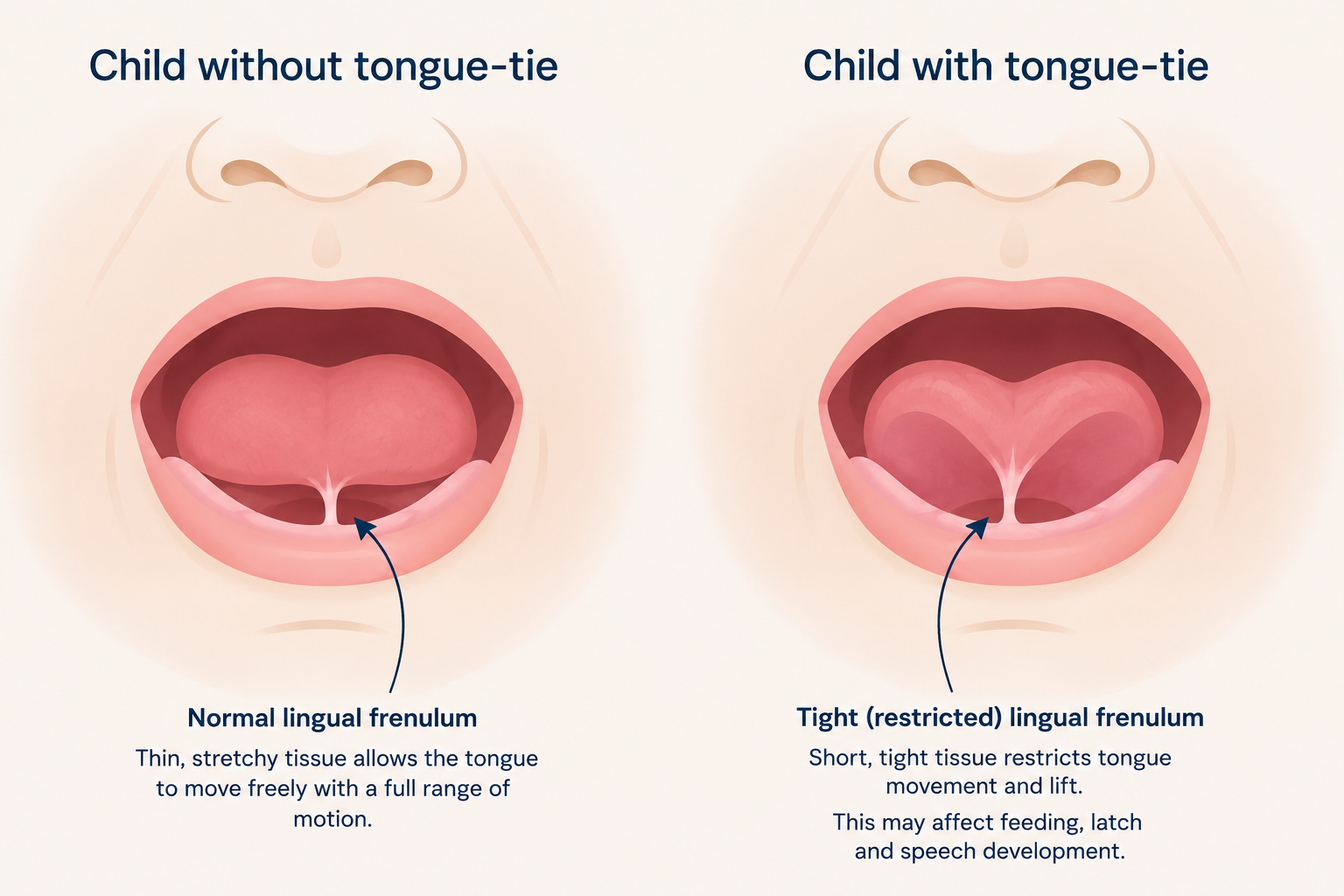
A tongue tie, known medically as ankyloglossia, occurs when the frenulum, the band of tissue connecting the tongue to the floor of the mouth, restricts normal tongue movement.
However, not every baby with a tongue tie will experience feeding difficulties. The tongue plays a crucial role during feeding. It needs to elevate, extend and cup around the breast or bottle teat to create an effective seal and generate suction. When movement is restricted, babies often compensate using their jaw muscles, lips and neck muscles, which can create tension patterns throughout the body.
Understanding Anterior and Posterior Tongue Ties
Anterior tongue ties are the easiest to recognise. The frenulum attaches closer to the tip of the tongue and is often visible when the baby cries or lifts their tongue. In more significant cases, the tongue may develop a characteristic heart-shaped appearance because the tight frenulum pulls the centre of the tongue backwards. These are often the tongue ties most easily identified by healthcare professionals and are commonly treated within NHS tongue tie services.
Posterior tongue ties are less obvious. The restriction sits further back beneath the tongue and can be more challenging to identify. In our clinic, we commonly encounter babies who have been identified as having posterior tongue ties, often after feeding difficulties have persisted despite support and an initial assessment. The tongue may appear relatively normal at first glance, yet the restriction can still affect feeding mechanics.
Parents are often surprised to learn that approaches to posterior tongue ties vary considerably across the UK. Some NHS services will assess and divide posterior tongue ties where appropriate, whilst others focus primarily on more obvious anterior tongue ties. As a result, some families choose to seek a private opinion when symptoms persist and feeding remains challenging.
One area that continues to generate discussion amongst healthcare professionals is whether all posterior tongue ties should be regarded as clinically significant. Some clinicians recognise posterior tongue ties as an important contributor to feeding difficulties, whilst others question whether they represent a distinct condition in all cases. This debate exists because feeding is complex. A baby may have a tongue restriction, but they may also have tension through the jaw, neck and upper body that affects their ability to feed efficiently.
This is one of the reasons we always assess the whole baby rather than focusing solely on the appearance of the tongue.
Signs That a Tongue Tie May Be Affecting Feeding
The signs are not always obvious. Some babies continue to gain weight and appear to feed regularly, but feeding remains inefficient and exhausting for both baby and parent.
Parents may notice difficulty achieving or maintaining a latch, repeated slipping off the breast, clicking sounds during feeding or a tendency to take in excessive air. Babies may become windy, unsettled or uncomfortable after feeds. Some dribble milk while feeding, whilst others cough, splutter or seem unable to maintain a good seal around the nipple or teat.
Feeding sessions are often prolonged and frequent, leaving parents feeling that they are constantly feeding without seeing their baby become fully satisfied. In some cases, poor weight gain, reflux-like symptoms and persistent feeding difficulties lead families to seek further assessment.
The Impact on Breastfeeding Mothers
Whilst much of the focus naturally falls on the baby, tongue tie can have a significant impact on mothers too.
One feeding pattern we commonly observe in babies with tongue ties is a tendency to clamp down with their gums when feeding. Ideally, a baby's tongue should extend and cup around the breast, creating a seal and generating the suction needed for efficient milk transfer. When tongue movement is restricted, some babies are unable to achieve this effectively and instead compensate by using their jaw and gums to maintain their latch. This compensation can place considerable pressure on the nipple and surrounding tissues. It is often one of the reasons mothers describe breastfeeding as feeling pinchy, sharp or uncomfortable throughout a feed rather than becoming more comfortable as feeding progresses.
We regularly see mothers who are experiencing painful feeding, cracked nipples, nipple trauma, blocked ducts and recurrent mastitis. When milk transfer is inefficient, feeding can become increasingly stressful and exhausting. Some mothers begin to notice a reduction in milk supply, whilst others find themselves questioning whether they can continue breastfeeding at all.
It is also common for babies with tongue ties to swallow excessive amounts of air during feeding because they struggle to maintain an effective seal. This can contribute to wind, discomfort and unsettled behaviour after feeds, creating further challenges for both baby and parents.
One of the difficulties with breastfeeding is that time matters. Each day that feeding remains ineffective can place additional strain on both mother and baby. Milk supply is being established, nipples are recovering from repeated feeds, and parents are often functioning on very little sleep. This is why we always try to accommodate babies with feeding concerns as quickly as possible. When breastfeeding is struggling, every day counts.
What About Lip Ties?
Many parents have also heard of lip ties. A lip tie occurs when the tissue connecting the upper lip to the gum is tight or restrictive.
Lip ties are very common and many babies have them without any feeding difficulties whatsoever. However, in some babies a restrictive upper lip may contribute to latch problems, particularly when it exists alongside a tongue tie.
The evidence surrounding lip ties remains less clear than the evidence for tongue ties. For this reason, feeding assessments should always consider the whole baby and the feeding process itself rather than focusing on any single structure in isolation.
Can Osteopathy Help?
This is one of the most common questions we are asked.
Osteopathy does not remove a tongue tie. However, it can help address the tensions and compensatory patterns that often develop around it.
Babies with feeding difficulties frequently present with tension through the jaw, neck, shoulders and upper back. We also commonly find asymmetry related to positioning in the womb or strains associated with the birth process. By improving mobility and reducing tension throughout the body, some babies are able to feed more effectively without requiring a tongue tie division.
In other cases, osteopathy forms part of a wider management plan. Sometimes we provide treatment before a tongue tie assessment, and sometimes we see babies after a tongue tie release to help them adapt to their new range of movement.
Not every tongue tie requires division. Some restrictions are mild and may improve significantly with feeding support, osteopathic treatment and time. Others continue to cause significant feeding difficulties despite conservative management and may benefit from further assessment by an experienced tongue tie practitioner.
Where Can You Have a Tongue Tie Divided?
Tongue tie division, often referred to as a frenulotomy, is available through many NHS services. Depending on the area, assessments and treatment may be provided by specialist infant feeding teams, midwives, ENT departments, paediatric surgical teams or dedicated tongue tie clinics.
Access and waiting times vary considerably across the country. Some families are seen very quickly, whilst others may face longer waits. When feeding difficulties are significantly affecting breastfeeding, some parents choose to seek a private assessment in order to access support more rapidly.
At The Waterside Practice, we work closely with a trusted network of local infant feeding professionals, including lactation consultants and experienced private tongue tie practitioners. Over the years we have developed strong professional relationships with colleagues who share our commitment to evidence-informed, baby-centred care. When we feel a baby may benefit from additional feeding support or specialist tongue tie assessment, we can help families access the appropriate services quickly. Equally, when a tongue tie has been divided, we often provide follow-up osteopathic treatment to help babies adapt to their new range of tongue movement and support the best possible feeding outcomes.
Looking Beyond the Tongue
Perhaps the most important message for parents is that tongue tie is rarely just about the tongue.
Every baby is different. Some babies with significant tongue ties feed perfectly well, whilst others with relatively mild restrictions struggle considerably. Feeding is influenced by many factors, including tongue function, body tension, birth history, feeding technique and maternal factors.
As osteopaths, we see babies every week whose feeding difficulties are influenced by a combination of these factors. Sometimes a tongue tie division is the right answer. Sometimes manual therapy and feeding support are enough. Most commonly, the best results come from looking at the whole baby and supporting both baby and parent through what can be a very stressful and emotional period.
If feeding is painful, exhausting or simply does not feel right, trust your instincts and seek support early. The sooner feeding difficulties are addressed, the better the outcome is likely to be for both mother and baby.
Further Reading and References
For parents wishing to learn more about tongue tie, breastfeeding difficulties and infant feeding support, the following resources provide balanced and evidence-based information:
• NHS. Tongue-tie. Available at: https://www.nhs.uk/conditions/tongue-tie/
• NHS Best Start for Life. Tongue-tie and breastfeeding. Available at: https://www.nhs.uk/best-start-in-life/baby/feeding-your-baby/breastfeeding/breastfeeding-challenges/tongue-tie/
• La Leche League GB. Tongue Tie. Available at: https://laleche.org.uk/tongue-tie/
• Hill RR et al. The prevalence of ankyloglossia in children aged under one year: A systematic review and meta-analysis. International Journal of Paediatric Dentistry. 2021. This review estimated the prevalence of tongue tie at approximately 8% of infants, although prevalence varies depending on the diagnostic criteria used.
• Borowitz SM. What is tongue-tie and does it interfere with breastfeeding? Current Opinion in Pediatrics. 2023. This review discusses the relationship between tongue tie and breastfeeding difficulties and highlights the complexity of diagnosis and management.
• Francis DO et al. Treatment of Ankyloglossia and Breastfeeding Outcomes. This review found evidence that frenotomy may improve breastfeeding and maternal nipple pain in appropriately selected babies, whilst also highlighting the need for further high-quality research.
A Note About Evidence
Tongue tie remains an evolving area of infant feeding research. Whilst there is good evidence that some babies with tongue tie experience significant feeding difficulties, there is ongoing debate regarding diagnosis, particularly in relation to posterior tongue ties, and which babies are most likely to benefit from division procedures. For this reason, assessment should always consider the whole feeding picture, including tongue function, feeding mechanics, maternal symptoms, lactation support and the baby's overall wellbeing.